Today’s guest post is written by Sarah Lohman, author of Eight Flavors: The Untold Story of American Cuisine (Simon & Schuster, 2016). On Monday, June 5, Lohman will give her talk, “The History of Garlic: From Medicine to Marinara.” To read more about this lecture and to register, go HERE.
Ms. Amelia Simmons gave America its first cookbook in 1796; within her pamphlet filled with sweet and savory recipes, she makes this note about garlic: “Garlickes, tho’ used by the French, are better adapted to the uses of medicine than cookery.” In her curt dismissal, she reflected a belief that was thousands of years old: garlic was best for medicine, not for eating. To add it to your dinner was considered the equivalent of serving a cough syrup soup.
There are records of ancient Greek doctors who prescribed garlic as a strengthening food, and bulbs were recovered from Egyptian pyramids. Garlic was being cultivated in China at least 4,000 years ago, and upper class Romans would never serve garlic for dinner; to them, it tasted like medicine.
In medieval Europe, garlic was considered food only for the humble and low. While those that could afford it imported spices like black pepper from the Far East, lower classes used herbs they could grow. Garlic’s intense flavor helped peasants jazz up otherwise bland diets. It was made into dishes like aioli, originally a mixture of chopped garlic, bread crumbs, nuts and sometimes stewed meat. It was intended to be sopped up with bread, although it was occasionally served as a sauce to accompany meats in wealthier households.
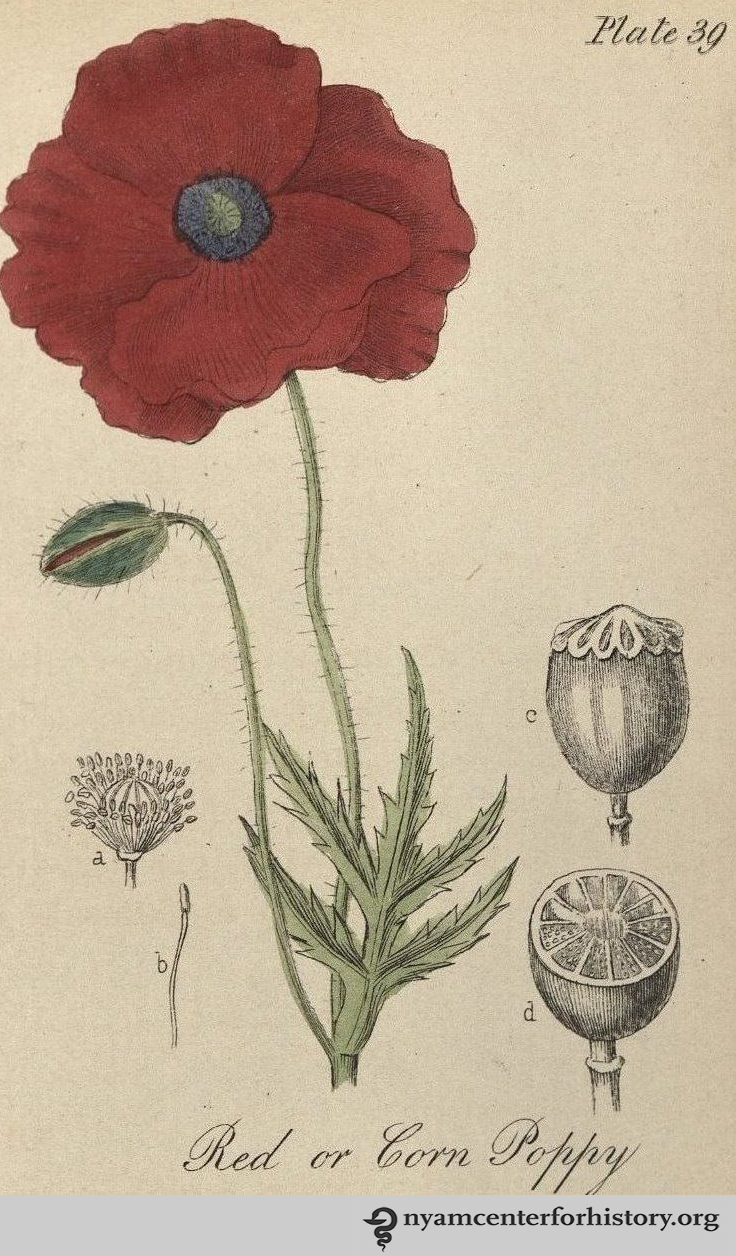
Garlic (Scientific name Allium Sativum) from Medical Botany (1790) by William Woodville.
The English, contrary to the stereotype about bland British cooking, seemed particularly enchanted by garlic. In the first known cooking document in English, a vellum scroll called The Form of Cury, a simple side dish is boiled bulbs of garlic. Food and medicine were closely intertwined in Medieval Europe, and garlic was served as a way to temper your humors. Humors were thought to be qualities of the body that affected on your health and personality. Garlic, which was thought be “hot and dry,” shouldn’t be consumed by someone who was quick to anger, but might succeed in pepping up a person who was too emotionally restrained. According to food historian Cathy Kaufman, a medieval feast might have a staggering amount of different dishes, all laid on the table at one time, so that different personality types could construct a meal that fit their humors.
Up through the 19th century, people also believed you got sick by inhaling bad air, called “miasmas.” Miasmas hang out by swamps, but also by sewage, or feet–I always imagined them as the puddles of mist that lie in the nooks between hills on dark country roads. Garlic can help you with miasmas, too. Ever see an image of plague doctors from Medieval Europe wearing masks with a long, bird-like beak? The beak was filled with odorous herbs, garlic likely among them, designed to combat miasmas.
In 18th-century France, a group of thieves may have been inspired by these plague masks. During an outbreak of the bubonic plague in Marseilles in 1726 (or 1655, stories deviate), a group of thieves were accused of robbing dead bodies and the houses of the deceased and ailing, without seeming to contract the disease themselves. Their lucky charms against the miasmas? They steeped garlic in vinegar, and soaked a cloth or a sponge in the liquid, then tied it like a surgical mask over their mouth and nose. In their minds, the strong smells would repel miasmas. This story is probably a legend, but I think there is some grain of truth to it: in modern studies, garlic has been shown to obfuscate some of the human smells that attract biting bugs. Since we now know bubonic plague was carried by fleas, it’s possible the thieves were repelling the insects. The plague is also a bacterial infection, and both vinegar and garlic are effective antimicrobials.
Garlic remained in the realm of medicine for most of the 19th century. Louis Pasteur first discovered that garlic was a powerful antimicrobial in 1858. In 1861, John Gunn assembled a medical book for use in the home, The New Domestic Physician, “with directions for using medicinal plants and the simplest and best new remedies.” Gunn recommends a poultice of roast garlic for ear infections:
“An excellent remedy for earache is as follows: Take three or four roasted garlics, and while hot mash, and add a tablespoonful of sweet oil and as much honey and laudanum; press out the juice, and drop of this into the ear, warm, occasionally.”

Garlick from Botanologia: The English Herbal (1710) by William Salmon.
He also recommends garlic for clearing mucus from the lungs and reducing cough, given by the spoonful with honey and laudanum. Gardening for the South: Or, How to Grow Vegetables and Fruits, an 1868 botanical guide, says the medicinal values of garlic include making you sweat, which, like bloodletting, was believed to leach out disease; it will also make you urinate, and is an effective “worm destroyer,” for any intestinal hitchhikers you might have. By the late 19th century, scientists also used garlic to treat TB and injected it into the rectum to treat hemorrhoids.
Today, garlic is one of the most heavily used home remedies, and it is increasingly being studied in the medical field. Some of its historic uses have been proved as bunk–while others, like its efficacy as a topical antiseptic, hold up. But since the late 19th century, garlic has found an even more worthwhile home, thanks to French chefs and Italian immigrants, who spread their garlic heavy cuisine around the world, and made even garlic-reticent Americans a lover of this pungent plant.
Join us on Monday, June 5 to learn more about this topic. Click HERE to register.