Today we have a guest post written by Ms. Julie M. Powell, 2018 recipient of the Audrey and William H. Helfand Fellowship in the History of Medicine and Public Health. Ms. Powell is a PhD candidate at The Ohio State University, her dissertation topic explores the growth of wartime rehabilitation initiatives for disabled soldiers and the rhetoric that accompanied and facilitated this expansion.
In May 1917, one month after the United States joined the First World War, the American Red Cross created the Institute for Crippled and Disabled Men to “build up re-educational facilities which might be of value to the crippled soldiers and sailors of the American forces.”[1] To this end, Director Douglas McMurtrie (1888–1944) collected approximately 3,500 separate books, pamphlets, reports, and articles from the European continent, North America, and the United Kingdom and its Dominions. He and his research staff pored over the documents, authoring reports, news articles, and lectures that were subsequently fed back into circulation both in the United States and abroad. A look at the collection and the work of the Institute provides a window into the development of rehabilitative care in the early twentieth century, demonstrating that transnational medical networks operated and expanded throughout the war and that the transmission of information and ideology often went hand in hand.

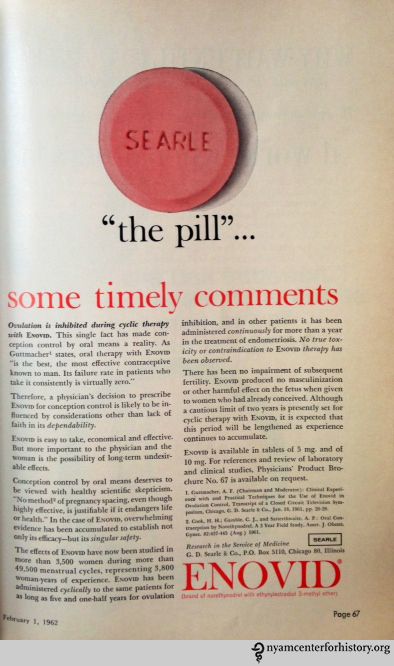
The Red Cross Institute for Crippled and Disabled Men, 1918.
The proliferation of literature on rehabilitation (including surgical amputation, orthopaedics, prosthetic design, physical therapy, and vocational re-education) can be attributed both to a sense of urgency—20 million men were wounded in the war—and to the relative newness of the field. The first orthopaedic institute was created in Munich in 1832 and the next in Copenhagen in 1872 but these, and others that followed, focused exclusively on care for disabled children. The first significant moves toward the retraining of adults were taken up in the two decades before the war. In 1897, in Saint Petersburg, disabled men began to be trained in the manufacture of orthopaedic devices and in 1908, with the founding of a school in Charleroi, Belgium, the industrially maimed were taught bookbinding, shoe repair, basket making, and more. The first retraining school for invalided soldiers was created in December 1914 in Lyon, France, four months after the outbreak of hostilities. The school provided the inspiration for over 100 similar schools throughout France. The period 1915–1917 saw a proliferation of orthopaedic and re-education institutions throughout Europe and the western world. It was on these models that the Red Cross Institute was founded.
The first institution of its kind in the United States, the Red Cross Institute for Crippled and Disabled Men resided at 311 Fourth Avenue (now Park Avenue South) in New York. Disabled men, either funded by the U.S. Army or attending through no-interest loans, trained in four trades: welding, mechanical drafting, printing, and the manufacture of artificial limbs. McMurtrie and his staff hosted meetings of disabled men—punctuated by cake and ice cream—wherein testimonials from the recently rehabilitated served as recruitment tools for the Institute.
But the broadest impact of the Institute came from its crusade to spread what McMurtrie referred to as the “gospel of rehabilitation”—an insistence on returning the disabled man to independence and self-sufficiency that he might eschew charity and compete fairly in the labor marketplace. Such notions were deeply rooted in classical liberalism, a foil to large-scale social welfare programs that would only emerge in the wake of the Second World War. In The Disabled Soldier, McMurtrie wrote plainly:
When the crippled soldier returns from the front, the government will provide for him, in addition to medical care, special training for self-support. But whether this will really put him back on his feet depends on what the public does to help or hinder, on whether the community morally backs up the national program to put the disabled soldier beyond the need of charity… In light of results already obtained abroad in the training of disabled soldiers, the complete elimination of the dependent cripple has become a constructive and inspiring possibility. Idleness is the great calamity. Your service to the crippled man, therefore, is to find for him a good busy job, and encourage him to tackle it. Demand of the cripple that he get back in the work of the world, and you will find him only too ready to do so.[2]

A reproduction (right) of part of McMurtrie’s poster exhibit for the Institute featuring the liberal “gospel of rehabilitation”: self-sufficiency, competition, and independence from charity.
McMurtrie’s gospel sounded the same notes as the works of U.S. Allies across the pond, whose material he’d spent years collecting. In 1918, famed novelist, advocate of the war wounded, and editor for the rehabilitation journal Reveille, John Galsworthy warned against the perils of charity, of “drown[ing] the disabled in tea and lip gratitude” and thereby “unsteel[ing] his soul.” Rather, he wrote:
We shall so re-create and fortify…[the disabled soldier] that he shall leave hospital ready for a new career. Then we shall teach him how to tread the road of it, so that he fits again into the national life, becomes once more a workman with pride in his work, a stake in the country, and the consciousness that, handicapped though he be, he runs the race level with his fellows, and is by that so much the better man than they.[3]


Such rhetoric was of a piece with appeals from British Minister of Pensions, John Hodge, for the restoration of men to “industrial independence,” that they might “hold their own in the industrial race.”[4]
When McMurtrie invited the world’s newly-minted experts in rehabilitation to New York in 1919, they shared—as they had through pamphlets, pictures, and films—not just information but ideology. Discussions on war surgery and the organization of rehabilitation schemes unfolded side-by-side with talks on public education and encouragement of the disabled to train.
Such propaganda efforts were critical. According to McMurtrie: “The self-respect of self-support or the ignominy of dependence—which shall the future hold for our disabled soldiers?” The credit or blame, he held, would rest with a public that either demanded self-sufficiency or patronized its men with charity.
References:
[1] Douglas C. McMurtrie, The Organization, Work and Method of the Red Cross Institute for Crippled and Disabled Men (New York: The Red Cross Institute for Crippled and Disabled Men, 1918).
[2] Douglas McMurtrie, The Disabled Soldier (New York: The Macmillan Company, 1919), 37.
[3] John Galsworthy, “Foreword,” The Inter-allied Conference on the After-Care of Disabled Men: Reports Presented to the Conference (London: His Majesty’s Stationary Office, 1918): 13–17. Reprinted in his book of essays Another Sheaf (New York: Charles Scribner’s Sons, 1919).
[4] John Hodge, “The Training of Disabled Men: How We Are Restoring Them to Industrial Independence,” Windsor Magazine no. 281 (1918): 569–571.
[5] McMurtrie, The Disabled Soldier, 75.