During the fall 2013 semester, Hunter College students in Professor Daniel Margocsy’s undergraduate seminar, Health and Society in Early Modern Europe, 1500–1800, visited NYAM several times to talk about rare anatomical books. Each student then studied one text in depth, learned about its bibliographical and historiographical context, and wrote a blog post about that item. We are pleased to feature two of the blog posts from the class, one last week and one today, both on books from our collections relating to midwifery.
By Rebecca Halff

The title page of Abrégé de l’art des accouchements. Click to enlarge.
Simply put, the magnitude of Angelique Marguerite Le Boursier du Coudray’s 1769 Abrégé de l’art des accouchements does not slap the reader in the face. The Abrégé is a small, light, unobtrusive volume. It easily fits in one’s hands and could be squeezed into a woman’s large apron pocket. Although it contains color images—a marker of luxury in eighteenth-century France—they are few, and are used only when illustrations are absolutely necessary. If we were to liken the midwifery textbook to a woman, we would say that despite her superior intelligence and great beauty, the Abrégé is modest and self-effacing, preferring to stand discretely in a corner at parties rather than flaunt herself ostentatiously.
This trait may be the reason the academic world neglected the Abrégé for so long despite its important contributions—and the important contributions of its author—to the field of midwifery. Only in 1998 was the first scholarly biography of du Coudray written.1 It is surprising that her unique story did not attract the interest of feminist historians before then. Not only was du Coudray a high-achieving woman of the eighteenth-century, but she gained fame when men were taking over the field of midwifery. This makes her quite an anomaly: she was a powerful woman in a field in which women were steadily losing power.2

Du Coudray, from the frontispiece of Abrégé de l’art des accouchements. Click to enlarge.
We know nothing about du Coudray’s first twenty years of life. She likely came from a middle-class background, but her only English-language biographer explains that “because we know nothing of her biological birth, her professional birth must serve as our beginning.”3We do know that at twenty-five years old, du Coudray had graduated from the College of Surgery in Paris and completed the three years of apprenticeship required to become an accredited midwife. Within the next few years, the school of surgery on the rue des Cordeliers, which had always welcomed midwives to its surgery lectures, decided to bar its doors to them. This was only one of many new developments that sought to exclude, reject, and ultimately eliminate female midwives. Du Coudray reacted by signing a petition pressing the Faculty of Medicine of the University of Paris to provide instruction to midwives and midwifery students.4
Surprisingly, University of Paris doctors conceded rapidly to the request. Their reasons for doing so have much to do with their age-old conflict with surgeons, a group of medical practitioners usually clustered into the same humiliating category as barbers. In 1743, however, the King had elevated the status of surgeons. Given their new prestige, surgeons sought to expand their territory to the field of midwifery, squeezing out female midwives by denying them instruction, as they had done at the school on the rue des Cordeliers. But Parisian midwives had challenged surgeons with their petition, arguing that their refusal to educate midwives amounted to neglect of their professional duties. Surgeons were accused of selfishly causing a dangerous reality: midwives were not being thoroughly trained, midwifery students were not becoming officially accredited, and as a result there was a shortage of midwives in the city. Doctors stepped in both to remedy the dilemma and to make their adversaries (surgeons) look worse than they already did.5

Plate III: A fetus in its natural position. Click to enlarge.
Through her involvement in this political matter, du Coudray gained a measure of renown in Paris. This was compounded by the very small number of midwives who were allowed to practice in the city—the world of Parisian midwifery was insular and intimate. Through what we today refer to as networking, Du Coudray made acquaintance and friends and formed alliances with important and well-connected medical professionals.
In 1759, King Louis XV charged du Coudray with the responsibility of educating rural midwives. In the wake of the Seven Years War, concerns had arisen over a high death toll and a simultaneous decrease in the French birth rate. Healthy pregnancies, safe deliveries, and the survival of infants suddenly became nationalist causes: France needed all the subjects it could get. The practice of midwifery became a means to support the state, and du Coudray soon became a national sensation and international symbol of French medical advancement.5

Plate XXIII deals with the difficulty of delivering twins presenting together and feet first. Click to enlarge.
At the King’s request, du Coudray began touring the French countryside to deliver medical lectures to rural midwives whose perceived incompetence was causing the deaths of French women (baby-makers) and infants (future soldiers and baby-makers). The Abrégé compiles these lectures in the order in which du Coudray delivered them. Du Coudray begins by discussing the female reproductive organs and the process of reproduction. She follows this with the issue of proper prenatal care. Finally, she instructs readers on deliveries, including how to handle common obstetric problems, for example a baby coming out feet-first, knee-first, stomach-first, or arm-first, the delivery of twins, and the delivery of a stillborn. Du Coudray concludes the Abrégé with a list of what she terms “observations”—singular cases that she believes should be noted despite their rare occurrence. These “observations” include the tale of a woman who remained pregnant for twenty-two months, and the case of a woman who began excreting the bones of a fetus as a result of an intestinal pregnancy.
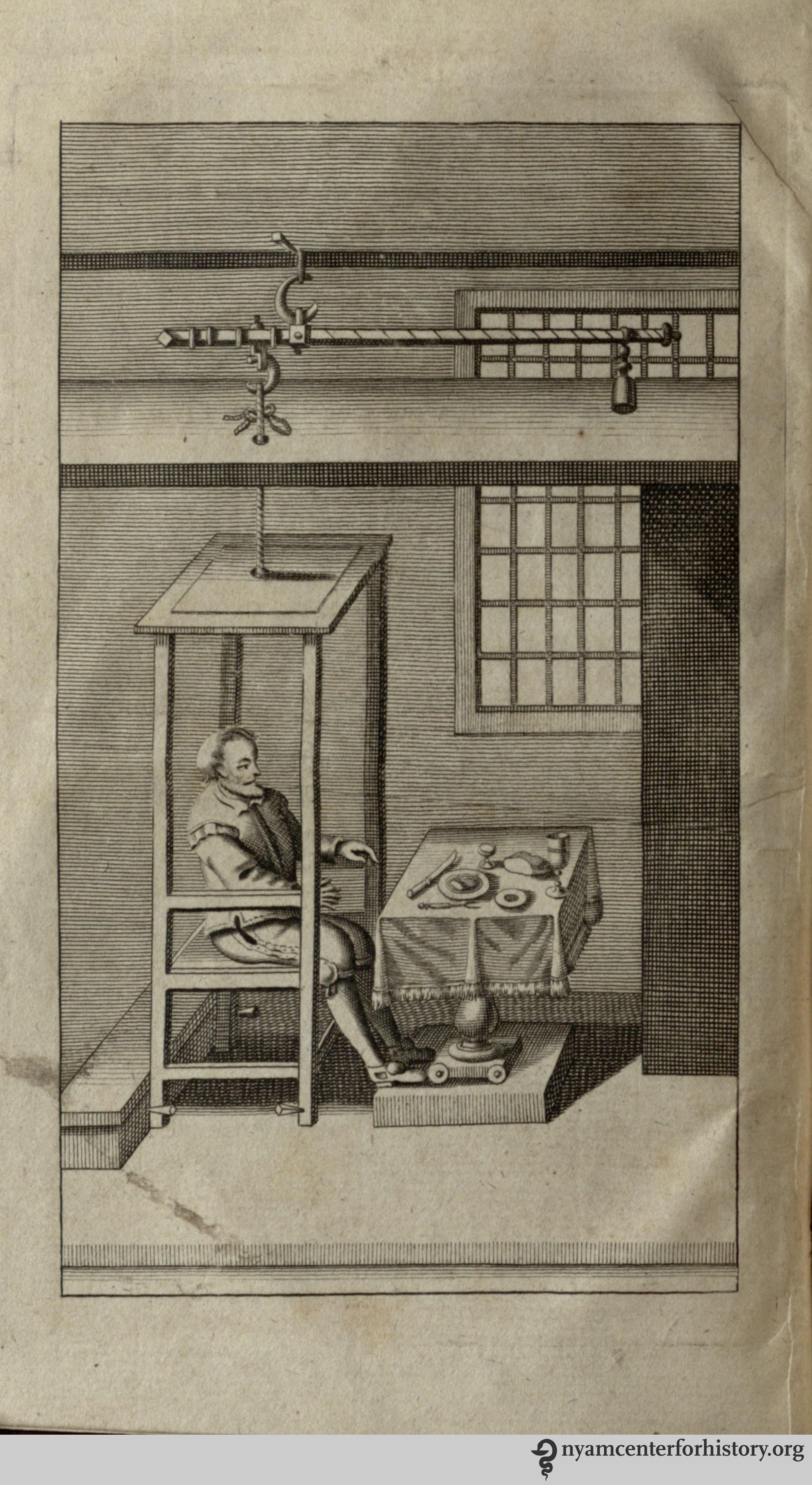
Du Coudray’s lecture series and the resulting Abrégé were incredible feats for an eighteenth-century woman. But the King’s midwife’s most celebrated achievement was not the publication of her book, but rather the invention of her “machine,” to which she refers several times in the Abrégé. This “machine” was the first of its kind: a teaching model of the female reproductive system. It came with a leather and cloth fetus which could be placed in any number of different positions to simulate the complications of a real delivery.

Picture of Madame du Coudray’s “Machine,” from Les Musees en Haute-Normandie.
Du Coudray was a medical innovator—a forward-thinking, idealistic pioneer. She realized the need for outreach to and instruction of rural midwives, toured France’s smallest villages to deliver these lectures herself, converted her lectures into a book format, and invented an anatomically accurate “machine” to ensure the proper training of midwives before they provided medical care.
But du Coudray did not stop her discussion at prenatal care and delivery. She also denounced traditional midwifery practices that caused unnecessary deaths, offering new ideas that would result in healthier mothers and babies. For example, du Coudray criticized the common practice of removing near-dead infants from their mothers immediately, done in order to avoid distressing the already exhausted and weakened new mother. These babies—immediately seized up as lost causes—were placed as far away from their mothers as possible, often on the floor. Midwives would then take care of their adult patient, leaving the baby to slowly perish. As du Coudray tells it, midwives could prevent many of these deaths if they did not give up on feeble infants so quickly and casually. Once, she recounts, she noticed that a baby’s toe had been bitten off by the household dog without anybody even noticing. Du Coudray accuses midwives of causing needless and preventable deaths through their foolish and antiquated practices. She instructs them to immediately attempt to revive faltering babies rather than leave them to their death.
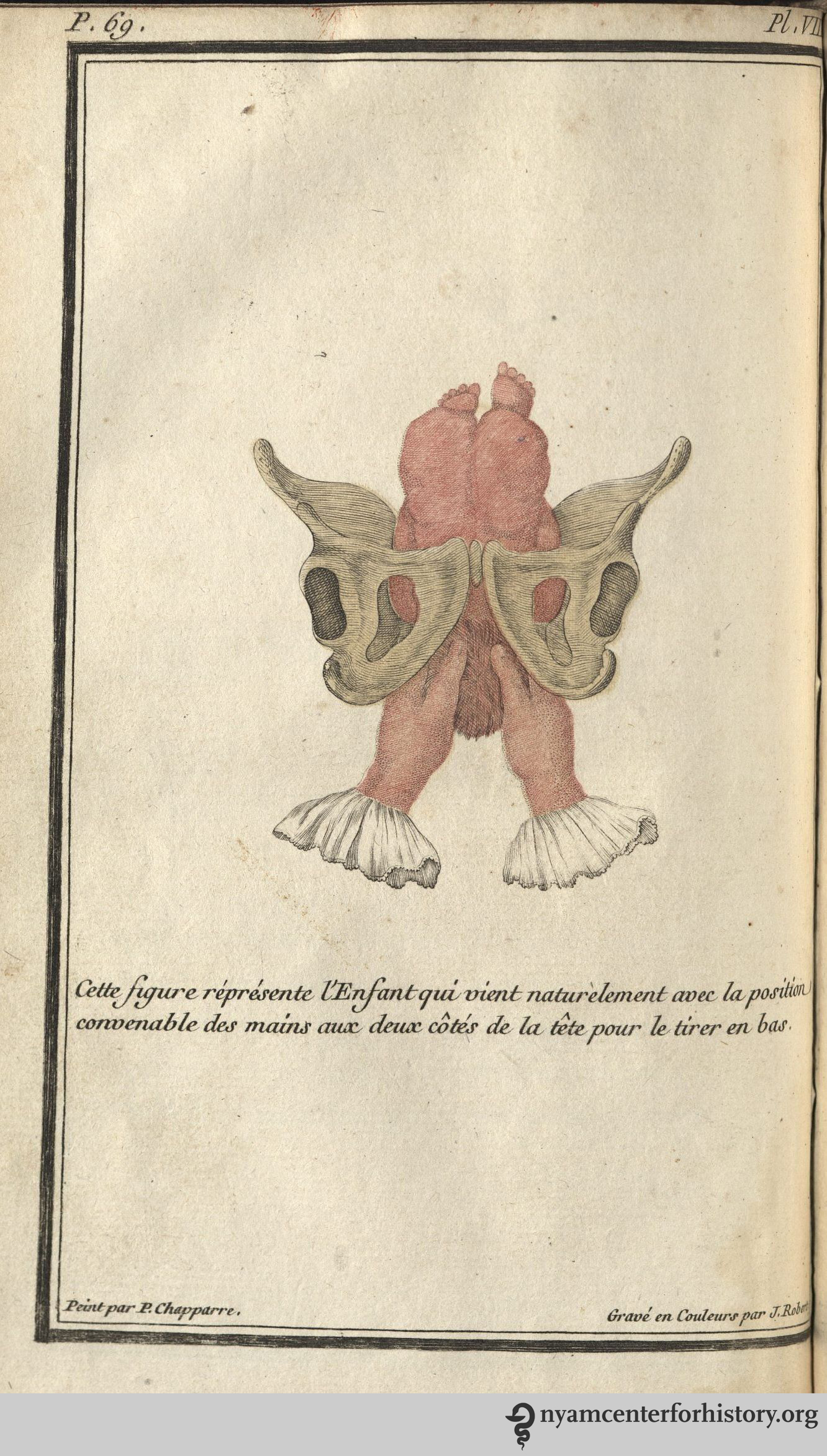
Plate VIII: The proper hand position to help the baby’s head emerge in a normal delivery. Click to enlarge.
Du Coudray was serious about her life’s work. She was simultaneously a medical innovator, concerned with advancing medical knowledge and developing new techniques, and a spokesperson for rural women who did not have access to competent midwives. But du Coudray does not present herself as either a medical innovator or a champion for ethical medicine in the Abrégé. Instead of proclaiming her passion for medicine, du Coudray downplays her agency, explaining again and again that she had no choice but to become involved in this work. Sometimes, she uses Christian rhetoric: how can we not, as good Christians, respond to the call of our brothers and sisters who need our help? Sometimes, she justifies her work by reframing it as nationalist—isn’t it a crime against France to deprive the nation of a subject? And sometimes, she cites the ineptitude of some midwives as the catalyst for her career: because of her intelligence, her natural duty is to find a way to transmit knowledge to someone with less knowledge. She even explains her greatest innovation in these terms, stating that she “perfected a machine which pity made [her] imagine.”
Like the Abrégé, du Coudray herself is self-effacing. A serious midwife who dedicated herself to her work, she cites religion, responsibility to the state, and pity for inspiring her career. Undoubtedly, she relied on this technique to get away with being a serious physician in a time when women were being pushed out of the medical sphere. She softened her persona and message to make it acceptable to male ears. But this technique did not die out with du Coudray. Women throughout history have used excuses to justify their pursuit of higher education and higher status, and will continue to do so until it is no longer necessary. Du Coudray provided the medical world with important resources, her book and her “machine.” She also left women with an example of how to achieve despite societal expectations, as she successfully gained a career she was passionate about, the mastery of her art, the esteem of her colleagues, students, and superiors, and a degree of fame and celebrity.
References
1. Nina Rattner Gelbart, The King’s Midwife: A History and Mystery of Madame du Coudray (Berkley and Los Angeles: University of California Press, 1998), 8.
2. Lisa Forman Cody, “Sex, Civility, and the Self: Du Coudray, d’Eon, and Eighteenth-Century Conceptions of Gendered, National, and Psychological Identity,” French Historical Studies 24 no. 3 (2001): 379-407.
3. Nina Rattner Gelbart, The King’s Midwife, 25.
4. Ibid., 26-42.
5. Ibid., 42-46.
6. “News,” Middlesex Journal or Universal Evening Post (London, England), Sep. 12, 1772.