
By Paul Theerman, Associate Director, Center for the History of Medicine and Public Health
Does one have a “right to health”? And if so, what does that right entail? Access to healthcare? Access to all healthcare? Equality of health outcomes?
The debate in this country over passage of the Affordable Care Act brought to the fore the differing assumptions over a “right to health.” Yet since at least 1946, members of the United Nations have asserted the right to health as a fundamental global human right. The constitution of the World Health Organization “enshrines the highest attainable standard of health as a fundamental right of every human being.”1 This right was further stated in the Universal Declaration of Human Rights of 1948—framed as the right to a standard of living “adequate for health and well-being.”2 The right to health remains a formative principle in global health. For example, three of the UN’s eight Millennium Development Goals are explicitly health related, and all have a health component.3
Though this right to health reached its full flower in the mid-20th century, it originated some 50 years earlier. In the late 19th century, urban and industrial ills had pushed their way onto the political agenda across the western world. Many reformers thought that supporting political rights was not enough: social and economic rights needed to be affirmed as well. One of these thinkers was the New York City-based urban researcher William Harvey Allen. In a series of books, and most notably Civics and Health (1909), Allen laid out the reasons why health was a human right.4

“Necessary to Efficient Democracy,” the way that experience in schools and other institutions is brought to the public, in Allen, Civics and Health, 1909, p. 310.
Allen made granting the right to health the apex of moral development, both in the individual and the society. He placed “rights” as the last and best of the seven motivations for public health action, starting with instinct and ranging through commerce to humanitarianism.5 Indeed, to promote health Allen said one could not rely on the love of money or the joy of human sympathy: “So long as those who suffer have no other protection than the self-interest or the benevolence of those better situated, disease and hardship inevitably persist.”6 By society’s affirming the right to health, it acknowledged that the citizenry’s well being had a claim on its attention and resources, and it made itself accountable to provide it. “Health administration is incomplete until its blessings are given to men, women, and children as rights that can be enforced through courts, as can the right to free speech, the freedom of the press, and trial by jury,” wrote Allen. The political rights claimed in the eighteenth century meant little if one did not have the physical means to exercise them in the twentieth. Those “permanently incapacitated . . . cannot appreciate the privilege of pursuing happiness.”7
According to Allen, it was not that people did not know what to do to secure public health—for the most part they did. It was rather that the means were often shunted aside, a problem of enforcement—and hence his argument for health as a right! Allen looked to find the most practical way to correct health deficiencies, and as co-director of the city’s newly established Bureau of Municipal Research, he looked upon all of New York as a test site.8 Here, he turned his attention to the health of school children, “the best index to community health.”9 Determining the status of children’s health was a comprehensive way of judging the health of the whole community, as children from all ranks of the community were available to reformers, and the mechanisms were already in place to examine and collect data. Allen saw children’s health as the indicator, not just to the health of the city, but to the right to health. Much of his book was devoted to measuring as well as intervening in children’s health, in such ways as enforcing milk purity laws, quarantines for communicable diseases, and vaccination for smallpox. He was concerned with controlling germs, paying attention to eye and ear health, and promoting school play and physical education. He saw the health of teachers as crucial to that of their charges. And, as detailed in our earlier blog post, he supported removal of tonsils and adenoids.
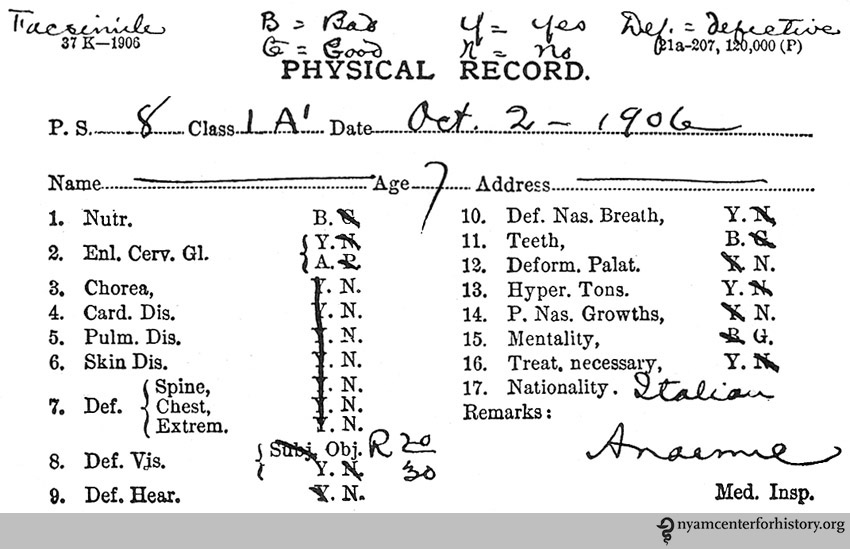
Sample record card for school physical examination, as found in Allen, Civics and Health, 1909, p. 34. As Allen noted: “Weight, height, and measurements are needed to tell the whole story.”
Yet, Allen did not think that the solution lay only in better school health. Society as a whole needed to address the health of its members throughout their lives. He suggested measures such as coordinating school health with other social agencies, requiring work physicals and promoting industrial hygiene, waging war on the “white plague” of tuberculosis, providing physicians with training not just in restorative medicine but also in preventive medicine, discouraging tobacco and alcohol use, and setting up institutions for large-scale information gathering and coordination through a national bureau of health.10
Many of Allen’s practical ideas today seem commonplace in the wake of the great shifts in public health that took place in the 20th century. But one thing stands out: seeing health as a right brought it out of the realm of enlightened self-interest and humanitarian relief. Health became social, health became enforceable, health became a right. That legacy, contested though it now is in American society, remains present today.
References
1. World Health Organization, Fact Sheet No. 323, “The Right to Health,” reviewed November 2013, http://www.who.int/mediacentre/factsheets/fs323/en/#, accessed September 23, 2015.
2. United Nations, “Universal Declaration of Human Rights,” Article 25, http://www.un.org/en/documents/udhr/, accessed September 23, 2015.
3. For the UN Millennium Development Goals, see http://www.un.org/millenniumgoals/, accessed September 23, 2015; for a summary of international conventions, see Mervyn Susser, “Health as a Human Right: An Epidemiologist’s Perspective on the Public Health,” American Journal of Public Health 1993 March; 83 (3): 418–26.
4. William Harvey Allen, Civics and Health, with an introduction by William T. Sedgwick (Boston, New York, Chicago, and London: Ginn and Company, 1909). For information on Allen (1874–1963), see in addition to the Recchiuti book below: “Reminiscences of William Harvey Allen: oral history, 1950,” Columbia Center for Oral History, http://oralhistoryportal.cul.columbia.edu/document.php?id=ldpd_4072329.
5. Allen, Civics and Health, pp 11–22. The seven motivations are Instinct, Display, Commerce, Anti-Nuisance, Anti-Slum, Pro-Slum [Abatement], and Rights.
6. Allen, Civics and Health, 20.
7. Allen, Civics and Health, 20.
8. For Allen and the Bureau of Municipal Research, see John Louis Recchiuti, Civic Engagement: Social Science and Progressive-Era Reform in New York City (Philadelphia: University of Pennsylvania Press, 2006), Chapter 4, pp. 98–124.
9. The phrase comes from the title of Chapter 4, “The Best Index to Community Health is the Physical Welfare of School Children,” page 33.
10. Allen, Civics and Health, Part III, “Coöperation in Meeting Health Obligations,” and Part IV, “Official Machinery for Enforcing Health Rights.” For an earlier attempt at a national bureau of health, see Jerrold M. Michael, “The National Board of Health: 1879–1883,” Public Health Reports 2011 Jan-Feb; 126(1): 123–29.
