Kate Mazza, today’s guest blogger, received her doctorate in US history from the Graduate Center, CUNY. Her dissertation, “The Biological Engineers: Health Creation and Promotion in the United States, 1880-1920” examines the ideas and progress of the interrelated health reforms of physical education and school hygiene. She has published an article, “Distracted At School: Aprosexia, ADHD and Adenoids in American Culture” in the Journal of American Culture.
 As the school year came to a close in June 1906, a panic swept through New York’s Lower East Side. According to newspaper reports, hundreds of parents, mostly Eastern European immigrants, ran to about a dozen local schools believing that their children were going to be harmed or murdered by doctors. Some people broke windows, some hit school workers, many yelled and cried and all demanded to see their children. At each school, children were eventually dismissed early, and, to the great relief of the frightened parents, were unharmed. A similar course of events took place in Brownsville, Brooklyn the next day.1 These events came to be known as the “adenoid riots” because they occurred a week after students had undergone surgeries, apparently without incident, to remove enlarged adenoids at Public School 110 in the Lower East Side.
As the school year came to a close in June 1906, a panic swept through New York’s Lower East Side. According to newspaper reports, hundreds of parents, mostly Eastern European immigrants, ran to about a dozen local schools believing that their children were going to be harmed or murdered by doctors. Some people broke windows, some hit school workers, many yelled and cried and all demanded to see their children. At each school, children were eventually dismissed early, and, to the great relief of the frightened parents, were unharmed. A similar course of events took place in Brownsville, Brooklyn the next day.1 These events came to be known as the “adenoid riots” because they occurred a week after students had undergone surgeries, apparently without incident, to remove enlarged adenoids at Public School 110 in the Lower East Side.
What caused the riots? Most accounts of the time blamed the immigrant population, stating that they were subject to panics, suspicious and ignorant of modern medical practice, and incensed and saddened by recent news of the Bialystok pogroms. Reporters also commented that local doctors intentionally spread rumors that children were being harmed because they saw free school and city services as a threat to their business.
Modern scholars, sympathetic to the immigrant’s perspective, have analyzed the events as a reaction against coercive means of assimilation.2 Yet while “Americanization” certainly played a role in this health initiative, school medical inspection affected children of all classes and ethnic groups in the United States and abroad. The confusion, fear, and misunderstanding of the adenoid riots was caused, in part, by erroneous beliefs about the implications of enlarged adenoids (masses in the back of the nasal cavity that can help fight infection), the methods used in NYC, and the zealousness of the hygienists to find and root out adenoids.
In 1887, Amsterdam physician A.A. Guye connected enlarged adenoids to aprosexia, or the inability to pay attention, along with poor memory and headaches.3 This idea laid the foundation for associating adenoids with academic failure, disobedience, and truancy. Over the years, physicians also linked enlarged adenoids to deafness, poor voices, trouble sleeping, colds, weight loss, restlessness, chest and mouth deformity, mouth breathing, ear disease, and even tuberculosis.4
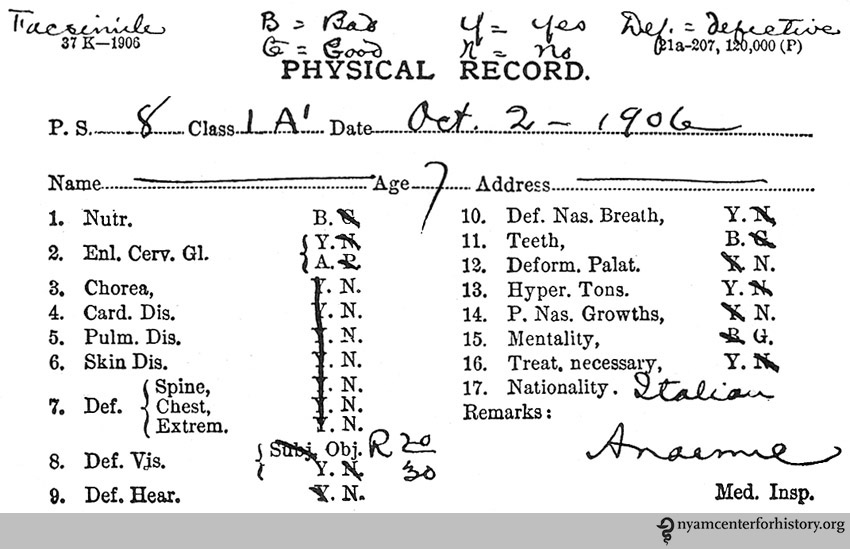
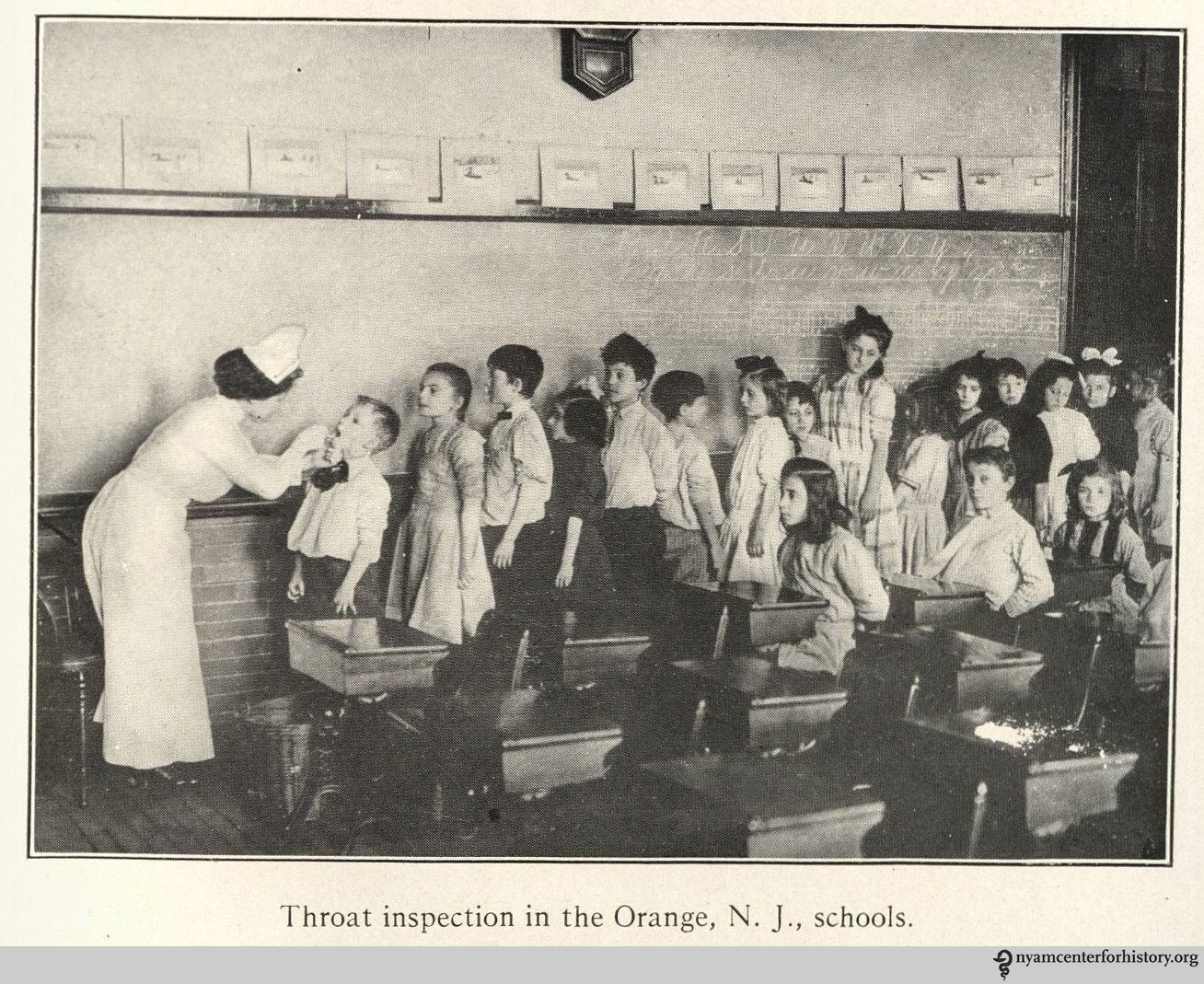
By the early 1900s, many involved in the growing school hygiene movement in the United States were convinced that enlarged adenoids were a common impediment to learning. In 1905 New York City became one of the first cities to inspect students for enlarged adenoids along with ear, nose, and throat problems. This more thorough physical examination was added to examinations for contagious diseases that had taken place since the 1890s in a number of cities.
Chief Medical Inspector of the New York City Department of Health, Dr. John C. Cronin, spearheaded the expanded medical inspection. He claimed that at PS 110, 137 children out of 150 in a specialized class of so-called “backward,” “incorrigible,” and “truant” children had enlarged adenoids.5 As the end of the school year approached, 56 children had had them removed, with 81 remaining. Cronin arranged to have the students convalesce in the countryside with the Society of Improving the Condition of the Poor at the end of the school year. Yet Cronin also wrote later that “it was then thought justifiable to get information as to what scholastic results would be obtained if these children were operated on collectively.”6 Seemingly frustrated, he brought in three doctors from Mount Sinai hospital to perform the operations at the school, after obtaining permission slips from parents. Cronin stated that doctors performed operations on 81 children in 84 minutes.7 While it was typical to do these surgeries quickly and without anesthesia or after care, these operations were done at an exceedingly rapid pace. From various accounts, children left the schools bleeding profusely. The riots occurred a week later.

“Mouth breathers immediately after ‘adenoid party.'” In Allen, Civics and health, 1909, p. 46.
Despite the rioting, Cronin publicized the efforts at PS 110 as an outright success. He held that all but four of the students had significant mental and physical improvement. He wrote: “From dullards, many of them have become the brightest among their fellows, after the operation.”8 A New Jersey doctor commented that removal of adenoids “has been followed by such wonderful improvement of the body and mind as to make recital sound like romance. The story of public school No. 110 in New York City, is almost beyond belief except to those who are familiar to it.”9 Medical and educational journals were filled with accounts of transformation through adenoid surgeries, many referencing PS 110.
As they preached their belief in transformation through surgery, these doctors and hygienists continually bolstered the idea that presence of enlarged adenoids caused poor scholarship and deviance. This association is clear when looking at hygiene statistics. When medical inspections took place in Northeastern urban centers, adenoids were found in roughly 30% of students. However, when the students were in a reformatory or a specialized class, like the students at PS 110, numbers climbed to 90%.
Even while the “adenoid craze” was in full swing, many parents did not abide by the prescriptions of medical inspectors to have their children undergo various treatments and adenoidectomy. When “defects” were found in school medical examinations, the rate of compliance was usually less than a third, as inspectors in various cities including Cleveland, Chicago, and Bridgeport, Connecticut remarked in the 1900s and 1910s.10
During the 1910s, the faith that experts had in the radical transformation of students through adenoidectomy began to wane. Walter Cornell, a leading advocate of the surgeries, found that his study group did not succeed academically after the surgeries as was expected, and wrote in 1912 that this case “certainly explodes the theory that the removal of adenoids is the panacea for all juvenile delinquencies.”11 Others began to see similar results.

“Typical adenoid faces showing mouth breathing, flattened noses, and protruding eyes.” In Gulick and Ayres, Medical inspection of schools, 1917 (2nd ed.), p. 170.
Medical inspection, particularly in New York City, came under fire, as many complained that examinations were too superficial and inaccurate and that enlarged adenoids were overdiagnosed. In one investigation, for example, the same group of children was examined by two different inspectors. The first inspector found that 70 students needed adenoidectomy, the second found that 96 did, with only 49 students in common.12
For school and city authorities, adenoid surgeries were an appealing, cheap, convenient way to reform education by changing the child, rather than overhauling the educational system. It is not surprising that they were overdiagnosed or misdiagnosed. While the adenoid riots took place at the beginning of the “adenoid craze,” they illustrate a general suspicion of these new hygiene practices and of the school’s new role in public health.
References
1. “East Side Parents Storm the Schools,” New York Times, 28 June 1906, pg. 4; “Throat-Cutting Rumors Revive School Rioting,” New York Times, 29 June 1906, pg.9.
2. For an interesting view of the adenoid riots, see Alan Kraut, Silent Travelers: Germs, Genes and the Immigrant Menace (Baltimore: Johns Hopkins University Press, 1994).
3. A.A. Guye, “On Aprosexia, Being the Inability to Fix the Attention and other Allied Alterations of the Cerebral Functions caused by Nasal Disorders,” Journal of Laryngology and Rhinology 3 no.11 (December, 1889):499-506.
4. For example, see Macleod Yearsley, Adenoids (London: The Medical Times, 1901); 39-74; W.E. Casselberry, “Facial and Thoraic Deformities Incident to Obstruction by Adenoid Hypertrophy in the Naso-Pharynx,” Journal of the American Medical Association 15 no. 12(September 20, 1890): 417-420; W.L. Grant, “Some Common Conditions of the Nose and Naso-Pharynx Demanding Operative Interference,” Philadelphia Medical Journal 2 no.16(October 15, 1898):798-799; Allen T. Haight, “Naso-Pharyngeal Adenoids as a Causative Factor in Ear Diseases,” Journal of the American Medical Association 33 no. 26 (December 23, 1899): 1577-1578.
5. John J. Cronin, “The Physical Defects of School Children,” The Journal of the New York Institute of Stomatology 2 no. 4(December, 1907):280.
6. Ibid., 280.
7. “Medical Attention in Public Schools,” American Gymnasia and Athletic Record 3 no. 6(February, 1907):125.
8. John J. Cronin, “The Doctor in the Public School” The American Monthly Review of Reviews 35 no. 4 (April, 1907): 438.
9. F.C. Jackson, “The Medical Supervision of Schools” The New Jersey Review of Charities and Corrections 7 no. 3 (March, 1908): 84.
10. Luther Gulick and Leonard Ayres, Medical Inspection of Schools (New York: Russell Sage, 1909, ed.), 102; Florence A. Sherman, “Medical Inspection in Bridgeport (Conn.) Public Schools,” Fourth International Congress on School Hygiene 4(August, 1913):394; Mrs. Edward W. Hooke, “To Save All Babies,” The American Club Woman 10 no. 6(December, 1915):117.
11. Walter Cornell, Health and Medical Inspection of School Children (Philadelphia: F.A. Davis Company, 1912), 278.
12. A Bureau of Child Hygiene: Co-operative Studies and Experiments by the Department of Health of the City of New York and the Bureau of Municipal Research (Bureau of Municipal Research, 261 Broadway: September, 1908): 13.