Lisa Rosner, PhD, author of today’s guest blog, will present “The True and Horrid Story of the Burke and Hare Anatomy Murders” at our October 18th festival, Art, Anatomy, and the Body: Vesalius 500.

Engraving of Dr. Robert Knox. From our online collection The Resurrectionists.
Dr. Robert Knox, the anatomist whose cadaver purchases kept William Burke and William Hare in the murder business, has always been an enigma. Born in Edinburgh, Scotland, he served in the army and studied in Paris before returning home to set up a private anatomical school. He taught hundreds of students, lecturing twice a day in addition to holding separate dissection classes. He was curator of the surgical museum, wrote articles on human and comparative anatomy for scientific societies, and was in the process of seeing several books on anatomy through publication. His supporters claimed he knew nothing about the murders; his detractors argued that he simply turned his blind eye—for he had lost an eye to smallpox as a child.

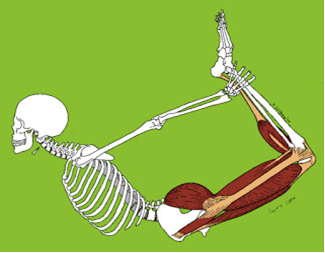
Plate II in Knox’s Man: His Structure and Physiology, shown flat and with lifted parts. Click to enlarge.
What we can see, using the extensive collection of Robert Knox materials in the New York Academy of Medicine Library, is just how talented an anatomist Robert Knox was. His edition of Hippolyte Cloquet’s A System of Anatomy is more than just a translation: it is instead a critical analysis of contemporary anatomical knowledge, enriched by examples from Knox’s own research and teaching. The same is true of his edition of Friedrich Tiedemann’s The Plates of the Human Arteries, prepared with two of his students, Thomas Wharton Jones and Edward Mitchell. The catalogue he prepared for the anatomical and pathological museum of the Royal College of Surgeons of Edinburgh is filled with his detailed insights: on anomalies of the biceps flexor cubiti, on the precise position relative of a fatal brain tumor, and on popliteal aneurism. Knox discussed the implications of these, and many more of his anatomical and surgical observations, in several series of articles for the London Medical Gazette. We can follow his teaching methods in The Edinburgh Dissector, the handbook he wrote for the use of his dissecting classes. “Nobody could ever say that he gave a dry lecture, or one that was not specially instructive,” reported his former student, Henry Lonsdale. Even in the midst of the detailed description that makes up most of the Edinburgh Dissector, Knox’s love of his subject shines through, as in his description of the bones of the foot, which “when well formed yields in beauty and perfection to no part in the human body.”
Could such a passionate observer of all subjects anatomical really have missed the fact that sixteen of his own “subjects” had been murdered? Contemporaries from Home Secretary Sir Robert Peel (founder of the London Metropolitan Police) to the Edinburgh evening papers refused to believe it and called for wider investigation. On the advice of legal counsel, Knox refused to answer any questions—just as he had refused to ask any, his professional rivals muttered darkly, when presented with Burke’s and Hare’s murder victims. There was no real case against him, and there are no records of any deliberations by the prosecuting attorneys. We will probably never know what Knox knew or when he knew it.

“Execution of the notorious William Burke the murderer, who supplied Dr. Knox with subjects.” Engraved print in The Resurrectionists collection. Click to enlarge.
The anatomical career of the talented Dr. Knox survived the Burke and Hare scandal, but it did not long survive the change in medical teaching and practices that followed it. He had a second career as a public teacher and lecturer: his books A Manual of Artistic Anatomy and Great Artists and Great Anatomists: A Biographical and Philosophical Study sold very well. But he never achieved the academic position he had striven for, and his research agenda, like his sixteen most famous subjects, died at the hands of Burke and Hare.
For more on Robert Knox and the Burke and Hare murders, visit our online collection, The Resurrectionists.