By Anne Garner, Curator, Rare Books and Manuscripts

Dr. John Thackery (Clive Owen) visits an opium den in The Knick. Cinemax, 2014
Dr. John Thackery passes through a number of dimly-lit opium dens in the heart of New York’s Chinatown during the course of The Knick. What were these dens really like—and who frequented them?
In the mid-19th century, the Chinatowns of America were largely isolated communities, populated by immigrants brought by labor brokers to work on the Central Pacific Railroad or other jobs. Many of these workers planned to return home after several years; there was little desire to assimilate. Scholar Gunther Barth has suggested that with the safety of a familiar culture came familiar vices.1
A large number of Chinese immigrants came from Canton, a region with a rich history of opium-smoking. As the Chinese presence spread east, opium dens cropped up in the Chinatowns of every major American city.
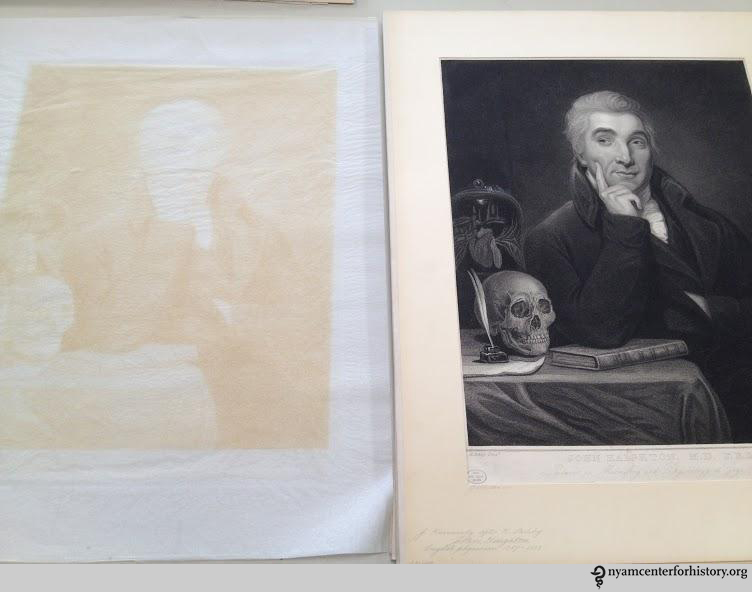
![American Opium-Smokers Interior of a New York Opium Den/ Drawn by J.W. Alexander. [New York] : Harper and Brothers, Oct. 8, 1881. Courtesy of Images from the History of Medicine (NLM).](https://nyamcenterforhistory.org/wp-content/uploads/2014/10/exhibition-ob10382.jpg?w=584)
American Opium-Smokers Interior of a New York Opium Den/ Drawn by J.W. Alexander. [New York] : Harper and Brothers, Oct. 8, 1881. Courtesy of Images from the History of Medicine (NLM).
The San Francisco ordinance coincided with an increasing anxiety among whites in large urban areas that the low-paid Chinese would threaten wages and standards of living. At the time, the country was mired in a deep recession. The federal Page Act, passed the same year as the San Francisco law, similarly targeted Chinese immigrants, aiming to “end the danger of cheap Chinese labor and immoral Chinese women.”3
Beginning with Virginia City the following year, local ordinances banning opium-smoking quickly passed across the U.S. These laws were largely ineffective. Law enforcement, focused on prosecuting Chinese dens known to attract white clientele, only drove whites deeper into Chinatown, and to smoke at higher rates.4
As opium use among whites increased, community leaders began to signal a concern about the morals of white women. Philadelphia missionary Frederic Poole cautioned that white women exposed by the Chinese to opium-smoking were at risk of “a life of degradation.”5 In 1883, Reverend John Liggins wrote of the dangers of the many New York City dens found in Mott and Pearl Streets (still the heart of Chinatown today), and quoted Kane that the habit, learned from the Chinese, contributed to “the downfall of innocent girls and the debasement of married women.”6 The same year, Allen S. Williams wrote in an early book on the opium-smoking habit about New York’s Chinatown dens:
Chinamen flit noiselessly by in ghostly, fluttering garments, and startle the Caucasian intruder by the very suddenness of their unsympathetic companionship…. the Chinese opium joint…is run for the sole purpose of pandering to a vicious taste whose indulgence is injurious to society.7
On the left coast, The Wasp, a popular San Francisco paper, sent two “reporters” to that city’s Chinatown in 1881, and published their findings:
In reeking holes ‘two stories’ underground, where the light of heaven and healthy atmosphere never penetrate, we found human beings living—if it may be called living, which is at best but an existence—as contentedly as rats in a sewer, whose habitation theirs so much resembles. The opium smokers’ resorts were among the first visited…a person once there, he may well desire to make himself oblivious of such surroundings and raise himself to a temporary heaven of his own, but how white men, and even white women, can bring themselves to descend to such filthy holes, where the reeking slime courses down the walls and the air is heavy with foetid odors, is a mystery to any well-regulated mind.8
The Wasp article offers an especially disturbing example of how many Americans implicated the Chinese as a group with standards and moral habits far inferior to those of whites. As early as the 1880s, opium dens run by the French and even white American-born women could be found in New York and Philadelphia, but the imagery continued to portray them as exclusively Chinese-owned and -operated. “It’s a poor town now-a-days that has not a Chinese laundry, and nearly every one of these has its lay-out [pipe plus accessories],” wrote one white traveler in 1883.9

Fig. 2—Smoker’s Outfit. In Opium-Smoking in America and China.
The framing of opium smoking as a Chinese problem continued as the century drew to a close. Temperance advocates and moral reformers identified opium smoking with indolence and passivity, qualities out of sync with a culture that emphasized hard work and a fast-paced industrial society. These kinds of characterizations became an important way to generate public revulsion for an immigrant group perceived to threaten both economic and social stability, and to gain traction for legislative action.10
The antagonisms toward the Chinese and attendant immigration restrictions resulted in a Chinese immigrant population that decreased by 1920 to less than half of what it was in 1890.11 The last opium den in New York was raided in 1957. Decades before, many of Chinatown’s dens, largely abandoned because of the rise of opium derivatives morphine and heroin, had all but disappeared.
References
1. Courtwright, David. Dark Paradise. Opiate Addiction in America before 1940. Cambridge: Harvard, 1982. 68.
2. Kane, H.H. Opium-Smoking in America and China. New York: G.P. Putnam’s, 1882. 1.
3. Peffer, George Anthony. Forbidden Familes: Emigration Experiences of Chinese Women Under the Page Law, 1875-1882. Journal of American Ethnic History, Vol. 6 No. 1, Fall, 1986.
4. Courtwright, 79.
5. Courtwright, 78.
6. Liggins, John. The Spread of Opium-Smoking in America. New York: Funk & Wagnalls, 1883. 20.
7. Williams, Allen Samuel. The Demon of the Orient and his Satellite Fiends of the Joints. New York: [the author], [1883]. 12.
8. The Chinese in California, 1850-1925.
9. Courtwright, 73.
10. Musto, David F. The American Disease. Origins of Narcotic Control. New Haven: Yale, 1973. 294-300.
11. Courtwright, 85.